Page contents
The NHS in Cornwall and the Isles of Scilly and the UK Health Security Agency (UKHSA) are extremely well prepared for outbreaks of new infectious diseases. The NHS has put in place measures to ensure the safety of all patients and NHS staff while also ensuring services are available to the public as normal. Read the latest guidance on COVID-19 for healthcare professionals
What is infection prevention and control?
Our infection prevention and control programme is led by our nurse consultant directors of infection prevention and control. Healthcare associated infections (HCAI) can occur as a result of healthcare or contact with healthcare environments. HCAIs arise across a wide range of clinical conditions and can affect people of all ages. They can worsen existing or underlying conditions, delay recovery and adversely affect quality of life. They can occur in otherwise healthy people, especially if invasive procedures or devices are used. Healthcare workers, family members and carers are also at risk of acquiring infections when caring for people.
A number of factors can increase the risk of acquiring an infection, but high standards of infection prevention and control practice, including providing clean environments, can minimise the risk. It is estimated that 300,000 patients a year in England acquire a HCAI as a result of care within the NHS. More than four million people in Europe acquire a healthcare-associated infection (HAI) every year, of whom approximately 37,000 die as a direct result of the infection, for further information please see 2016 point prevalence survey for healthcare associated infections, antimicrobial use and antimicrobial stewardship in England.
Measles
Vaccination rates have fallen, and cases of measles are increasing in England. Large outbreaks have occurred.
This document provides advice for clinical and non-clinical staff in general practice.
Key points are:
- Ensure staff readiness to recognise, segregate, assess and report possible or probable cases.
- Any patient with fever and a rash is potentially infectious.
- Staff without evidence of immunity may be excluded from work if assessed to be contacts.
- There is a national campaign to promote MMR and practices should consider their capacity to respond to potential increases in MMR requests.
This poster from the UK Health Security Agency contains more information on measles for A+E, walk-in and GP centre healthcare workers.
The Kernow Health CIC Cornwall primary care training hub delivers a monthly “Primary Care Spotlight” podcast that brings you all the latest news and insights from the hub. The infection prevention and control team were invited as guests on the podcast in March 2024 for a measles episode. Please listen to the podcast on your preferred platform by visiting the Kernow Health CIC primary care spotlight webpage.
Is your practice ready?
To assess the readiness of your general practice, please complete the NHS CIOS ICB Measles…are you ready? questionnaire.
Measles guidance
Please refer to relevant guidance:
- UKHSA National Measles Guidance
- Risk Assessment and Infection Prevention and Control Measures for Measles in Healthcare Settings
- Appendix 1: Practical steps towards completing a local risk assessment for measles in healthcare settings
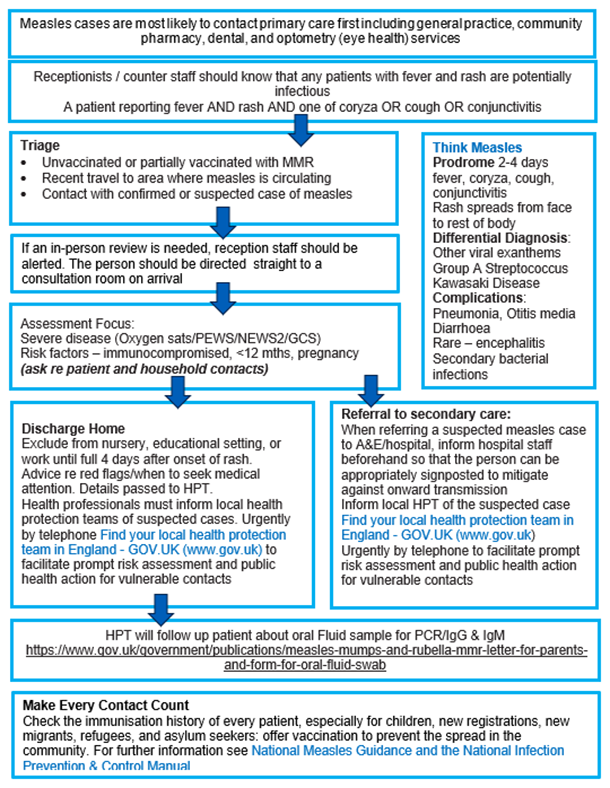
- Appendix 2: Think Measles – primary care actions for screening, triage and management
- The Green Book chapter 21: Measles
- PPE when assessing/treating suspected or confirmed measles cases
- Primary care mask selection poster
{kind=link}
FAQs
How can I report a suspected measles case?
UKHSA Notifiable diseases poster (publishing.service.gov.uk)
How do I test for measles?
How is Measles prevented?
What are the signs and symptoms of measles?
Measles starts with a 2 to 4 day “prodromal” phase before the rash appears, with coryza, cough, conjunctivitis, and a fever.
fever typically increases, to peak around rash onset.
rash generally starts behind the ears, spreads to the face, and then expands onto the trunk and can become generalised. The rash is red, blotchy, maculopapular (not itchy) and lasts around 3 to 7 days.
the rash is more difficult to spot on dark skin.
Koplik spots may appear around the time of the rash and last for 2 to 3 days so can easily be missed. They are small white or bluish/white lesions on the buccal mucosa. They can be confused with other lesions in the mouth and so their suspected presence is an unreliable marker of measles.
the infectious period spans 8 days i.e. cases are infectious from 4 days before rash onset and for 4 full days after.
several other common rash illnesses have similar presentations (especially in young children) e.g. roseola, parvovirus infection and scarlet fever, and so identification on clinical features alone may be unreliable.
What are the complications of measles?
- Pneumonia or bronchitis
- Convulsions
- Diarrhoea
- Meningitis or encephalitis
- Immune thrombocytopenic purpura (ITP)
- Late-onset subacute sclerosing panencephalitis (SSPE).
Who is at risk of measles?
- Unvaccinated individuals
- Pregnant women
- Immunocompromised patients
- Chronically ill patients
Is there any treatment for measles?
How is measles spread?
How long are people with measles contagious?
How do I prepare my practice for measles?
immunisation status/records are available for all staff (clinical and non-clinical) that may be exposed to a suspected or confirmed case of measles and staff are supported to ensure they are fully immunised. Satisfactory evidence of protection would include documentation of having received 2 doses of MMR or having had a positive antibody test for measles. Please be aware that Health care workers who are exposed to a confirmed or suspected case of measles and do not have satisfactory evidence of protection (2 documented doses of measles containing vaccine or measles IgG positive) should be excluded from work from the 5th day after their first exposure to 21 days after the final exposure. For occupational health measures, please see Section 2.6 of Guidance for risk assessment and infection prevention and control measures for measles in healthcare settings
patient screening, triaging and testing protocols are in place for all relevant care settings to ensure prompt isolation of suspected or confirmed cases of measles. All staff undertaking a reception and triage role, should be trained and fully aware of the questions to be asked when talking to patients requesting an appointment, especially those who report, fever, coryza or cough, conjunctivitis, and rash. Please note that some symptoms are experienced before the rash appears but are still infectious. Please see Appendix 2: Think Measles – primary care actions for screening, triage and management.
a respiratory season or winter plan is in place to ensure, for example, appropriate segregation of patient cases depending on the pathogen and management of increasing case numbers where they occur.
FFP3 respirator fit testing is completed for staff who may be required to assess or clinically care for a suspected or confirmed measles case. Please see Fit2Fit RPE Fit Test Providers Accreditation Scheme and Fit Testing in the UK – RPA for all your Fit Testing needs for fit testers.
training in IPC measures is provided to all staff, including: the correct use of PPE and the correct technique for donning and doffing (putting on and removing) PPE safely. Please see NHSE national infection prevention and control manual chapter 2.4 Personal protective equipment (PPE) and respiratory protective equipment (RPE)
risk assessment(s) is undertaken for staff who may be at high risk of infection and/or complications from infection with measles.
Make every contact count by ensuring patients visiting your practice have their immunisation status checked and offered MMR if appropriate.
What are the recommendations for respiratory protection and FFP3 masks?
As standard infection prevention practice, line with the health and safety at work act (1974), the personal protective equipment at work regulations (1992) and the health and social care act (2012), all healthcare providers should implement a robust internal system that ensures all staff caring for patients with a suspected confirmed pathogen spread wholly or partly via the airborne route have the appropriate respiratory protective equipment (RPE); the poster When do I need to wear a mask? Information for primary care can support mask selection, and for a more comprehensive guide, the respiratory protective equipment section of NHSE national infection prevention and control manual chapter 2: Transmission based precautions.
Please note that staff must be fit tested with FFP3 masks annually to ensure the masks offer any protection to the wearer. There will be a mask to fit everyone, but not everyone will fit every mask due to variations in facial structure, which can change over time (the rationale behind regular fit testing requirements). Please see HSE fit-testing basics for further information.
Please see Fit2Fit RPE Fit Test Providers Accreditation Scheme and Fit Testing in the UK – RPA for all your Fit Testing needs for fit testers.
What are the recommended infection prevention and control precautions?
If remote consultation is not possible, or, if following telephone triage, the patient is advised to attend your primary care setting, please ensure a separate entry area and uncluttered consulting room with a window can be used (if possible) as this allows for minimal transmission within your practice and for the area to be ventilated and all surfaces cleaned following the visit. Please note: If your practice has air conditioning and the air is re-circulated you should also turn this off during the visit, again to reduce risk. Please also see the Harrogate patient placement and assessment for infection risk policy for general practice – which lists the requirements for isolation listed below and the Harrogate safe management of the care environment policy for general practice – which lists requirements for cleaning and disinfection processes.
An identified room or designated area should be used for isolation.
A notice should be displayed on the door stating, ‘Isolation area – no unauthorised entry’.
The room should be free from clutter and, where possible, equipment not required for the consultation should be removed from the room before the patient enters.
Always use SICPs and TBPs.
Ensure appropriate personal protection equipment (PPE) is available, e.g. disposable aprons, gloves, facial protection. RPE is required for suspected or confirmed airborne pathogens please see primary care when do I need to wear a mask?
Ensure hand hygiene facilities are available, e.g. wall mounted liquid soap, paper towels, wall mounted alcohol hand rub or in a pump dispenser.
A foot operated lidded waste bin with a liner should be available and waste disposed of as infectious waste.
Medical devices and care equipment used in the room should be disposable. If reusable items are used, they should be appropriately decontaminated before removal from the room.
Do not use linen pillowcases and ‘modesty’ blankets, couch roll should be used. If a pillow is used, it should be encased in a cleanable plastic case.
Where possible, ensure good ventilation by opening windows.
The isolation room or area used for isolation should be decontaminated, i.e. cleaned, and disinfected, after use. If the room cannot be decontaminated immediately, a notice should be displayed stating ‘Isolation area – awaiting deep clean, do not enter’.
PPE required for confirmed or suspected cases is:
FFP3 mask or respirator, that the individual has been fitted for, please see above section for further information.
Apron
Gloves
Eye protection
Please see some examples of high-level disinfectant products:
Clinell clorox wipes
PDI sani-cloth Chlor wipes
Clinell peracetic acid wipes
Chlor-Clean tablets
Actichlor Plus tablets
For it to be effective, fogging requires stringent cleaning prior to using the machine, so settings should not rely on fogging alone.
Should a patient require an inter health and social care transfer, please inform the ambulance service and admitting department, to ensure the appropriate actions and isolation facilities are available when the patient arrives.
How long should a clinical treatment room be left before cleaning following vacation of a suspected/confirmed case of measles?
In hospital settings, the majority o general wards/single rooms should have at least 6 ACH, the fallow times required in these settings is a minimum of 20 minutes. If the air changes within the room/area are unknown or known to be lower than 6 ACH, the fallow time should be extended.
Measles virus can survive in the air for up to 2 hours, if the ACH in a room are unknown this can be used to guide decision making regarding fallow times.
What recommendations should I give patients suspected of having measles?
What are the current recommendations for measles vaccination?
Can I test staff immunoglobulin G (igG)?
What are the recommendations for measles post-exposure prophylaxis (PEP) and isolation?
First, notify the South West Health Protection Team (HPT) (UKHSA) immediately when a case is suspected. Please see section ‘how can I report a suspected measles case?’ above for further information.
Following your notification to UKHSA and if the case is confirmed or thought to be likely measles, you may be asked to follow-up on known exposures in your practice. The key priorities are outlined below.
The National Guidelines for Measles outlines the public health actions for healthcare settings and healthcare workers following exposure by a case of measles, and provides advice on the assessment for PEP for vulnerable contacts who are exposed to measles.
When a known exposure has occurred within a healthcare setting, the key priorities are as follows:
- Identify when (date and times) and where the case attended the setting, in addition to all locations attended and movements within the setting e.g. different rooms, areas, wards, toilets, canteens.
- Identify which patients and those attending with patients, members of the public and/or staff (including volunteers) may have come into contact (as defined in section 3) with the case within the healthcare setting.
- Determine if any person who encountered the case, is in a vulnerable category and requires PEP.
- Confirm if staff or volunteers who encountered the case, have documented evidence of 2 doses of measles, mumps, or rubella (MMR) vaccination or previous measles infection (confirmed by measles IgG test).
When a suspected or confirmed case of measles has attended a healthcare setting, contact tracing efforts should prioritise the identification of these vulnerable contacts and a risk assessment for each of these identified contacts should be undertaken.
Contact tracing should focus on all patients and those attending with patients, members of the public, e.g. visitors/contractors and all staff (including volunteers).
The risk assessment for each identified vulnerable contact and the recommended follow-up action, will depend on their exposure risk and their likely susceptibility.
‘Contact’ with a likely or confirmed case of measles is defined by the National Measles Guidelines as:
- close contacts including household contacts
- face to face contact of any length
- spending more than 15 minutes in a small, confined area. For example, a 4-bed hospital bay, reception area, treatment room
Please see below suggested approach to contact tracing, with support available from UKHSA and system partners including the ICB IPC team:
- Confirm case’s period of infectiousness (i.e. 4 days before and 4 days after onset of rash, with rash as day 0). Confirm date(s) of the exposure event(s) within the healthcare setting, with UKHSA.
- Identify the timeline of the case’s movements within the healthcare setting during the exposure event(s). Investigate where, when and the length of time specific locations were attended e.g. reception area, triage, waiting room, ward, consulting room, chapel, restaurant/canteen, shop, pharmacy.
- Establish if the case had any contact or attended the same specific locations (regardless of exposure duration and size of room) with people who are immunosuppressed. If yes, assess the contact(s) susceptibility and identify actions required using the National Guidelines for measles.
- Establish if within 6 days from the exposure event, the case had face to face contact of any length or shared a small, confined space for >15 minutes with any pregnant women or infants <12 months. If yes, assess the contact(s) susceptibility and identify actions required using the National Guidelines for measles.
- If it is not clear who is vulnerable within a defined list of contacts and therefore not possible to conduct an individual contact risk assessment, a warn and inform letter and/or text should be sent to all potential contacts (in conjunction with UKHSA and system partners).
- Healthcare workers who are exposed to a measles case and do not have satisfactory documented evidence of protection (i.e. 2 doses of the MMR vaccine or previous measles infection), must be excluded from work. The required exclusion periods are outlined in the National Guidelines for measles.
- If following the contact risk assessment process, it is identified that follow-up actions are required e.g. administering PEP to vulnerable contacts, sending warn and inform messages, then please contact UKHSA.
Who can I contact with additional queries?
For general public health queries, please contact the public health team via phnotifications@cornwall.co.uk.
For further vaccination and immunisation queries, please contact the NHS CIOS ICB vaccination and immunisation team via email: ciosicb.vaccinations@nhs.net.
Should you have any infection prevention and control additional queries, please fill out Measles additional infection prevention and control queries
For urgent infection prevention and control (IPC) queries, please contact the IPC team via ciosicb.ipc@nhs.net
Additional Measles Resources
- MMR vaccinations for 17- to 30-year-olds
- MMR resources for general practice
- What to do if you think your child has measles and when to keep them off school
- Confirmed cases of measles in England by month, age and region: 2023
- NHS national infection prevention and control manual
- Practical steps towards completing a local risk assessment for measles in healthcare settings
- Guidance for risk assessment and infection prevention and control measures for measles in healthcare settings
- UKHSA National Measles guidelines
- Viral rash in pregnancy
- NICE Clinical Knowledge Summary – Management of measles
- MMR training slide set for immunisers (found under the vaccination subheading)
- Think Measles! UKHSA poster
- YouTube Measles: how infectious is it compared to other illnesses?
- Green Book chapter 21: Measles
- Fit2Fit RPE Fit Test Providers Accreditation Scheme
- Fit Testing in the UK – RPA for all your Fit Testing needs
Collaboration
Close collaboration with local acute and community trusts as well as neighbouring trusts and commissioners ensures monitoring and improvement is shared.
Commissioning expectations
We expect the services we commission to comply with specific regulations. In relation to infection prevention and control the expectation is that services will be delivered as set out in The Health and Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance, more commonly known as The Hygiene Code.
All services registered with the Care Quality Commission are required to declare compliance with a specific standard relating to infection prevention and control and this relates directly to the Hygiene Code.
In addition to these standards there are additional annual improvement expectations relating to some infections. These are set by NHS England and included in our contracting processes.
Hospitals
Our local hospitals all have their own infection prevention and control teams and details of their work can be found at the links below:
- Cornwall Partnership NHS Foundation Trust – Infection Control
- North Devon District Hospital
- Plymouth Hospitals NHS Trust
- Royal Cornwall Hospitals NHS Trust
We engage with the infection prevention and committees and/or steering groups of these organisations.
Expectations specific to infection prevention and control are embedded within our contracts with providers and evidence of compliance is checked every month.
Infection prevention and control network
View our download our Infection prevention and control network poster
Developing the confidence and competence of local health and social care providers in identifying and managing IPC risks and promoting good antimicrobial stewardship are key priorities within national IPC guidance. A Cornwall IPC network will support implementation of effective IPC practices with full support from the NHS Cornwall and Isles of Scilly IPC team. The network is not intended to replace specialist IPC practitioners however, the aim is to have at least one connection in each primary care and care home setting across Cornwall and providers can nominate as many individuals as they like to sign up to the network. The network is currently structured in three free of charge training levels as outlined below.
IPC champions
The champion level delivers a six-month course based on a workbook, currently offering 8 sessions. This level is reserved for care home staff only with both clinical and non-clinical job roles
IPC link practitioners
The link practitioner level delivers a six-month course, currently offering 14 sessions. This level is reserved for clinical staff in primary care and care home settings only.
Train the trainer
A trainer the trainer level will be developed in due course, with more information to follow.
Monthly Newsletters
Monthly email newsletters with current IPC updates are sent to all who would like to be included on our email distribution list.
Contact information
For further information or to sign up to the IPC champion or link practitioner programmes or monthly email newsletters, please contact the NHS infection prevention and control team via email: coisicb.ipc@nhs.net
YouTube presentations
The infection prevention and control team have developed narrated presentations on YouTube to support providers with implementation of processes. Please see links below:
Hand hygiene training and audit guidance
The national standards of healthcare cleanliness 2021 implementation guidance
Antimicrobial resistance
Antimicrobial resistance (AMR) arises when the micro-organisms which cause infection survive exposure to a medicine that would normally kill them or stop their growth. This means that the treatments usually used to treat infections caused by a resistant organism will not be effective.
Many of the medical advances in recent years, for example organ transplantation and cancer chemotherapy, need antibiotics to prevent and treat the bacterial infections that can be caused by the treatment. Without effective antibiotics, even minor surgery and routine operations could become high risk procedures if serious infections can’t be treated.
The UK government published a 20-year vision for AMR in January 2019. Some key information from this document is shown below.
- No poverty: AMR strikes hardest on the poor; treatment of resistant infections is more expensive.
- Zero hunger: Untreatable infections in animals threatens sustainable food production for growing populations.
- Good health and wellbeing: Antimicrobials are fundamental components of all health systems.
- Clean water and sanitation: Reduces infections and antibiotic residues from multiples sources contaminate water.
- Decent work and economic growth: Cost of AMR is predicted to be US $100 trillion by 2050, driving an extra 28 million people into poverty.
- Responsible consumption and production: It is crucial to balance access and conservation of antimicrobials with innovation, to contain AMR.
The World Bank estimates that an additional 28 million people could be forced into extreme poverty by 2050, through shortfalls in economic output, unless resistance is contained.
The 20-year vision for AMR
By 2040, the vision is of a world in which AMR is effectively contained and controlled through strong mitigation.
The UK is determined to sustain its efforts to:
- combat resistance
- taking local, national and global one-health approaches across humans, animals, the environment and food
This is in line with global ambitions and in collaboration with other nations, partners and the international community.
In our vision, stakeholders at local, national and global levels are:
- collectively strengthening policy and practice
- ever improving understanding through research and surveillance
- developing effective regulation and advocacy to contain and control resistance
In the UK, we will contribute to the global effort through:
- a lower burden of infection, treatment of resistant infection and minimised transmission in communities, the NHS, farms, the environment and all other settings
- optimal use of antimicrobials and good stewardship across all sectors, including access to the safe and effective medicines that have been manufactured responsibility or all who need them, achieving usage levels, by sector, as good as the best countries in the world where comparable data is available
- new diagnostics, therapies, vaccines and interventions in use, and a full AMR research and development pipeline for antimicrobials, alternatives, diagnostics, vaccines and infection prevention across all sectors
Local AMR work
In response to the first UK national strategy in 2013 a Cornwall antibiotic resistance group (CARG) was convened.
Purpose of the group
- Responsible for ensuring implementation of UK 5-year AMR national action plan, specifically supporting delivery of 3 main strategic aims.
- Reports to health and wellbeing boards via health protection committee.
- Also reports into various committees within each stakeholder organisation. For example the medicines optimisation programme board.
Work streams
- Education and engagement with the public.
- Education and engagement with healthcare workers and vets.
- Comprehensive stewardship programme for all sectors.
Primary care
GP practices in Cornwall and the Isles of Scilly have been implementing the TARGET antibiotics toolkit:
- Treat
- Antibiotics
- Responsibly
- Guidance
- Education
- Tools
The toolkit aims to help influence:
- prescribers and patients personal attitudes
- social norms and perceived barriers to optimal antibiotic prescribing
It includes a range of resources that can each be used to support prescribers’ and patients’ responsible antibiotic use. Therefore helping to fulfil continuing professional development (CPD) and revalidation requirements.
Quarterly antibiotic prescribing data is sent out to GP practices, including data for individual prescribers. This data helps them to monitor their total antibiotic items and numbers of broad spectrum antibiotics that should be kept to a minimum because of AMR.
Education
An e-learning healthcare module on reducing AMR was launched in November 2015.
This module was designed to support all health and social care staff, both clinical and non-clinical, in a variety of settings. The module can help you understand the threats posed by AMR, and ways to tackle this major health issue. This programme has been developed by Health Education England in collaboration with Public Health England and NHS England.
Antimicrobial prescribing and stewardship competencies
The antimicrobial prescribing and stewardship competencies can be used by any independent prescriber and can help with the professional development of prescribing antimicrobials. There are 5 competencies:
- Infection prevention and control.
- AMR and antimicrobials.
- Prescribing antimicrobials.
- Antimicrobial stewardship.
- Monitoring and learning.
Care home resources
The infection prevention and control team at NHS Cornwall and Isles of Scilly provides a service for the care sector which includes
- A programme of education and training for IPC champions and link practitioners (please see details in IPC network section, or contact the team for more information)
- Support with cases of transmissible infection
- Developing IPC resources in line with national guidance, and offering support with their use
- Giving bespoke IPC advice on request
- Site visits to support with IPC audits
Our contact details are via email: ciosicb.ipc@nhs.net
For care home outbreak information and resources, please visit South West Councils: UKHSA infection prevention and control and winter readiness toolkit for care homes and other residential care settings. Please report all suspected or confirmed outbreaks to UKHSA via telephone: 0300 303 8162. To give updates for existing outbreaks, telephone: 0300 303 8162 or email swhpt@phe.gov.uk.
Care homes are required to register with the Care Quality Commission (CQC) and declare compliance with various standards. The care home annual report template has been designed to support providers in evidencing their CQC requirements, please email the infection prevention and control team if you would like support with using the template.
The standard that relates to infection prevention and control comes from the Health and Social Care Act 2008: Code of practice on the prevention and control of infections and related guidance, a document that is commonly referred to as the hygiene code.
Training
In addition to the IPC Network, and face-to-face bitesize training that can be added to a supportive audit site visit, the IPC team delivers virtual annual updates for care homes (held quarterly) via Kernow Health CIC. Please see poster for virtual annual IPC updates for care homes (held quarterly) for further information.
Useful links
- When do I need to wear a mask? Information for care homes
- Infection prevention and control: resource for adult social care
- Winter readiness pack for care homes 2023 to 2024
- Hydration assessment tools
- Hydration resource pack
- diarrhoea recording form
- Group A strep bitesize guidance
- Norovirus bite size guidance
- Adult social care residents with glutamate dehydrogenase positive toxin negative results bitesize guidance
- Clostridioides difficile infection bitesize guidance
- Scabies bitesize guidance
- Shingles bitesize guidance
- UKHSA PPE donning and doffing guidance
- RCHT pathology handbook
- UHP pathology handbook
- Royal Devon university healthcare pathology handbook
- Recognising urine infections can be difficult in older people. The UTI diagnostic tool should be used to assess symptoms and communicate with the GP
- NHS how to take a stool sample: This resource has been developed as part of the Midlands IPC Collaborative Group. The animation provides an overview of how to take a stool/faecal sample for service users who have diarrhoea/loose stools. The animation covers when samples should be taken and how to collect the sample, including how much of a sample is required. Reminding teams to be SIGHTED on the risks associated with diarrhoea and the importance of early sample taking.
Care Home Policies
Cornwall Council, on behalf of NHS Cornwall and Isles of Scilly ICB, procured the Harrogate and District NHS Foundation Trust Community Infection Prevention and Control Policies for Care Homes and disseminated them to all settings in the region in winter 2021. We endorse the use of these polices and have received very positive feedback from providers. We recommend settings ensure they have the correct versions in use within their setting by visiting the Harrogate and District NHS Community Infection Prevention and Control Care Home Policies webpage.
Care home cleaning
To support care homes to review their current processes to align with national standards, please see example care home cleaning specification template including functional risk categorisation, elements, performance parameters, cleaning frequencies and cleaning responsibilities.
National standards recommend using risk categories for different areas based on what happens there, and the categories then help decide how and how often things are cleaned. Please see NHSE the national standards of healthcare cleanliness 2021 to view the national standards. Further local guidance on using the standards can be found in the 18-minute YouTube narrated presentation the national standards of healthcare cleanliness 2021 implementation guidance.
Care Home audit and competency assessment tools
- care home audit calendar template
- Care home annual report template
- care home general audit tool (annual)
- hand hygiene competency assessment tool
- water safety audit tool
In our care home audit calendar template some of the audit tools and competency assessment tools we recommend using are provided by Harrogate and District NHS Foundation Trust Community Infection Prevention and Control. These are:
- Aseptic technique Policy for Care Home settings
- Aseptic technique procedure audit tool for care homes
- Commode and commode pan audit tool
- Enteral tube feeding competency audit tool
- Hand hygiene audit tool for care homes
- Mattress and mattress cover audit tool
- Personal protective equipment audit tool
- Pressure relieving cushion and cover audit tool
- Safe management of the care environment audit tool for care homes
- Safe management of care equipment audit tool for care homes
The Harrogate and District NHS Foundation Trust Community Infection Prevention and Control website offers a variety of useful additional resources to settings, please visit their website for further information Harrogate and District NHS Community Infection Prevention and Control resources for care homes.
Clinical care home support team
The clinical care home support team is a Cornwall Partnership NHS Foundation Trust support service to enhance care led by general practice, and the wider health care system. The team is available for virtual clinical advice and support, this can also include care setting site visits when appropriate. The team offers:
- education and personalised support in enhancing the health of your residents. Including training on recognising and managing deterioration with tools such as NEWS2 or RESTORE2
- supporting transitions of care out of hospital to care homes.
- clinical and pastoral advice and guidance
- shared clinical decision-making, risk management and shared clinical accountability
- support with monitoring of clinical conditions
- professional development of staff
- escalate unsafe staffing issues
- on-site clinical support if appropriate
- ongoing support for COVID-19
- navigating to other teams and clinical professionals
For non-urgent queries please contact the team via email on: cft.cchsn@nhs.net. For urgent queries, please see the 24/7 care home professionals’ line in the section below.
24/7 care home professionals’ line
The care home clinical assessment and support line is supported by NHS 111 (out of hours) and the care home support team (Monday to Friday 9am-5pm). This should not replace your normal route for first line clinical support via your GP.
Call the 24/7 care home professionals’ line on: 01872 303770
General practice resources
NHS Cornwall and Isles of Scilly provide data and learning opportunities for primary care, the resources below may be useful. The infection prevention and control team also offer site visits to practices to support with completion of a general IPC audit or deliver face to face bitesize training. Please email the infection prevention and control team: ciosicb.ipc@nhs.net to arrange a visit.
Microbiological testing
To help prevent specimen rejection and to ensure patients receive correct and timely treatment, please refer to your local pathology handbook below for information pertaining to specimen collection and analysis:
Handwashing
Personal protective equipment
Healthcare associated infections
- NICE: Healthcare-associated infections: prevention and control in primary and community care
- NHS how to take a stool sample: This resource has been developed as part of the Midlands IPC Collaborative Group. The animation provides an overview of how to take a stool/faecal sample for patients who have diarrhoea/loose stools. The animation covers when samples should be taken and how to collect the sample, including how much of a sample is required. Reminding teams to be SIGHTED on the risks associated with diarrhoea and the importance of early sample taking.
Guidelines and specifications
- The primary care annual report template has been designed to support providers in evidencing their CQC requirements, please email the infection prevention and control team if you would like support with using the template.
- Guidelines on the facilities required for minor surgical procedures and minimal access interventions
- NICE quality standard infection prevention and control
- NHS Improvement: Learning from patient safety incidents
- Safe management of healthcare waste (including colour codes)
- As part of preparing practices for the possible need to give intramuscular human normal immunoglobulin, please see UKHSA guide Immunoglobulin: when to use.
Training
In addition to the IPC Network for link practitioners, and face-to-face bitesize training that can be added to a supportive audit site visit, the IPC team delivers virtual annual updates for primary care (held quarterly) via Kernow Health CIC. Please see Poster for virtual annual updates for primary care (held quarterly) for further information.
Primary care spotlight podcast
The Kernow Health CIC Cornwall primary care training hub delivers a monthly “Primary Care Spotlight” podcast that brings you all the latest news and insights from the hub. The infection prevention and control team were invited as guests on the podcast in March 2022 and for a miniseries during infection prevention and control week in October 2022. Please listen to the podcasts on your preferred platform by visiting the Kernow Health CIC primary care spotlight webpage.
Primary Care policies
We endorse the use of the Harrogate and District NHS Foundation Trust Community Infection Prevention and Control Policies for General Practice and have received very positive feedback from providers who have purchased them for a small fee, as well as those who have downloaded the freely available versions. We recommend settings ensure they have the correct versions in use within their setting by visiting the Harrogate and District NHS Community Infection Prevention and Control Policies for General Practice webpage.
Primary care cleaning
To support primary care settings to review their current processes to align with national standards, please see example primary care cleaning specification template including functional risk categorisation, elements, performance parameters, cleaning frequencies and cleaning responsibilities.
National standards recommend using risk categories for different areas based on what happens there, and the categories then help decide how and how often things are cleaned. Please see NHSE the national standards of healthcare cleanliness 2021 to view the national standards. Further local guidance on using the standards can be found in the 18-minute YouTube narrated presentation the national standards of healthcare cleanliness 2021 implementation guidance.
Primary care audit and competency assessment tools
- primary care audit calendar template
- primary care annual report template
- primary care minor operations audit tool
- hand hygiene competency assessment tool
- water safety audit tool
In our primary care audit calendar template, some of the audit and competency assessment tools we recommend using are provided by Harrogate and District infection prevention and control. These are:
- Aseptic technique competency assessment record for general practice
- Aseptic technique procedure audit tool for general practice
- Hand hygiene audit tool for general practice
- National Standards of Healthcare Cleanliness audit scoresheet
- Personal protective equipment audit tool
- Safe management of the care environment audit tool for general practice
- Safe management of care equipment audit tool for general practice
The Harrogate and District NHS Community Infection Prevention and Control website offers a variety of useful additional resources to settings, please visit their website for further information Harrogate and District NHS Community Infection Prevention and Control resources For general Practice.
Healthcare associated infection learning from experience
In addition to ongoing routine surveillance, the infection prevention and control team review cases of healthcare associated infections. Learning is reported anonymously and shared at local forums; monthly slides are available on request: ciosicb.ipc@nhs.net for providers to share locally. Feedback is given directly to providers and individualised support offered as required. We welcome engagement, and thank you for your support. Please see healthcare associated infection learning from experience poster for further information.
Urinary Catheters
The CFT Urinary catheterisation in adults policy is available to use for all providers of health and social care in Cornwall. This guidance document sets out clinical advice relating to urinary catheterisation and catheter care in ensuring the highest standards of care and practice are consistently delivered across all services used by our patients; and to ensure providers meet clinical best practice standards in delivering direct patient care in urinary catheters/catheterisation.
Innovations in catheter care continue to be explored by many clinicians and scientists, especially to reducing catheter-associated urinary tract infection (CAUTI), catheter blockages and bladder mucosal irritation, which is vital to ensure safety and reduce harm (Jeffery and Mundy 2020).
In 2019 we launched our catheter passport. The passport was developed to be likened to a logbook for each resident to give them information on how to care for their catheter as well as a clinical section in the back for their nurses, doctors and carers to fill in as necessary.
Unfortunately, catheters can significantly increase the risk of urinary tract infections and whilst these infections are usually mild, they can on occasion be serious and can impact general health and wellbeing, which is what we’re trying to prevent.
The catheter passport also includes useful information including a pee-o-meter to ensure hydration.
Our aim is for them to be used county-wide throughout the NHS in Cornwall for anyone that has been fitted with a catheter. If you would like any information or require a supply of catheter passports email the infection prevention and control team We have produced bookmarks as part of a hydration project to provide a handy reminder to drink enough fluid and check urine for signs of dehydration. If you would like any information or would like a supply of bookmarks, email the infection prevention and control team
C. diff passports and #ThinkCdiff
To raise awareness of C. diff infection risk, prevention and management amongst patients, carers and health and social care workers, and to support patients with a diagnosis of C. diff to get the right care and treatment, a local C. diff passport, with an attached C. diff card, has been developed. Please see the C. diff case study for further information about the benefits for patients, carers, and healthcare workers. A #ThinkCdiff poster for general practice has also been developed as a reference guide for primary care practitioners.
If a patient receives a C. diff positive stool specimen result, they should be provided with a C. diff passport and verbal information on C. diff. The C. diff passport is designed for patients and/or carers to complete, with support from healthcare workers, if needed. The passport has been designed for patients to take to all health and social care appointments, so their infection risk can be communicated, and to support the right use of antibiotics, which is a significant risk factor for residents with C. diff. Please contact the IPC team if you would like free of charge copies of the passport, or should you have any queries: ciosicb.ipc@nhs.net
There is also a what is C. diff poster that can be displayed in health and social care settings to inform service users on the risks, signs and symptoms of C. diff
NHS how to take a stool sample: This resource has been developed as part of the Midlands IPC Collaborative Group. The animation provides an overview of how to take a stool/faecal sample for patients who have diarrhoea/loose stools. The animation covers when samples should be taken and how to collect the sample, including how much of a sample is required. Reminding teams to be SIGHTED on the risks associated with diarrhoea and the importance of early sample taking.
Water safety
Providers of health and social care premises statutory obligations for water safety are enforced by the health and safety Executive (HSE). The HSE Legionnaires’ disease technical guidance has lots of useful information and HSE control of legionella bacteria audit checklists (1 and 3) are also helpful. For detailed technical guidance on management of water systems in healthcare premises, please refer to:
- HSE Legionnaires’ disease. The control of legionella bacteria in water systems
- HSE Control of Legionella in hot and cold water systems in care services / settings using temperature
- Health technical memorandum (HTM) 04-01) Safe water in healthcare premises
For primary care settings, the CQC GP myth buster on legionella outlines expectations on legionella risk assessments and control measures.
UKHSA responding to the detection of legionella in healthcare premises describes when a healthcare premises should contact the UK Health security agency (UKHSA) health protection team (HPT). National guidance on Legionnaires’ disease is also available Legionnaires’ disease: guidance, data and analysis.
Settings with augmented care areas must ensure that the water quality is of a higher microbiological standard, which is dependent on both the type of service user and the augmented care areas intended use, as outlined in HTM 04-01 addendum Pseudomonas aeruginosa – advice for augmented care units.
There is no fixed definition of “augmented care”, but the description encompasses caring for service users with severe immunosuppression because of disease or treatment, including heavily immunosuppressed service users during high-risk periods in their therapy.
Infection prevention and control best practice guidance in water safety would be to include the following assessments in the practices regular water safety audit schedule:
- Has the practice undertaken an assessment by an approved water engineer?
- Is the practice undertaking the actions listed by the water engineer?
- Is water sampling being performed?
- Are weekly water temperature checks being performed at sentinel taps?
- Are flushes of little used outlets being performed at least twice weekly?
- Is there evidence of managing limescale?
- Is there evidence of quarterly cleaning, disinfection and limescale removal of showerheads?
- Have “dead legs” (water outlet in an unused area) been removed, if identified by the water engineer?
Please see our infection prevention and control water safety audit tool for use for primary care and care homes.
Whole system norovirus plan
Please see our whole system norovirus plan that articulates the collaborative approach of key organisational stakeholders in the local health and social care economy to manage the impacts of norovirus infection in Cornwall.
NHS how to take a stool sample: This resource has been developed as part of the Midlands IPC Collaborative Group. The animation provides an overview of how to take a stool/faecal sample for patients who have diarrhoea/loose stools. The animation covers when samples should be taken and how to collect the sample, including how much of a sample is required. Reminding teams to be SIGHTED on the risks associated with diarrhoea and the importance of early sample taking.
Patient information
MRSA
Further precautions at home if you have MRSA
Hand hygiene
Washing your hands is one of the easiest ways to protect yourself and others from illnesses such as food poisoning and flu. Washing your hands properly should take about as long as singing Happy Birthday twice (around 20 seconds). Use the following steps from the World Health Organisation while you hum:
- Wet your hands with water (warm or cold).
- Apply enough soap to cover all over your hands. You can use alcohol-based hand rub if you don’t have immediate access to soap and water.
- Rub hands palm to palm.
- Rub the back of your left hand with your right palm with interlaced fingers. Repeat with the other hand.
- Rub your palms together with fingers interlaced.
- Rub the backs of your fingers against your palms with fingers interlocked.
- Clasp your left thumb with your right hand and rub in rotation. Repeat with your left hand and right thumb.
- Rub the tips of your fingers in the other palm in a circular motion, going backwards and forwards. Repeat with the other hand.
- Rinse hands with water (warm or cold).
- Dry thoroughly, ideally with a disposable towel.
- Use the disposable towel to turn off the tap.
How often should we wash our hands?
We should wash our hands:
- after using the toilet
- after handling raw foods like chicken, meat and vegetables
- before eating or handling ready to eat food
- after having contact with animals, including pets
Why is it so important to wash hands properly?
Washing your hands properly removes dirt, viruses and bacteria to stop them spreading to other people and objects, which can spread illnesses such as food poisoning, flu or diarrhoea.
Washing your hands with soap and water is sufficient to remove dirt, viruses or bacteria and it can reduce the risk of diarrhoea by nearly 50%.
Who is most at risk from the effects of poor hand hygiene?
Children are particularly at risk of picking up infections and spreading them to other people. It’s especially important to make sure that hands are washed when you’re visiting someone in hospital or other healthcare setting, to help prevent the spread of infection.
Infections
How do infections spread?
You need a germ. The germ lives in or on its host, another person, an animal or a contaminated surface, for example a door handle, worktop or equipment.
The germ is passed on by either direct or indirect contact which can be coughing, sneezing, hand contact with someone who carries the germ on their hand or by touching a contaminated surface.
If the germ then enters your system and you’re not immune to it, you can catch the infection. Generally healthy people are less likely to catch infections, as their immune system should protect them well. But if for any reason your immune system is weaker than normal, you will be more vulnerable and therefore need to protect yourself even more against any infection.
Any infection can be caught or spread were there are ill people together, this can be in a hospital, a care home a GP surgery or in a public place. The information below explains how you can help the staff to reduce infection and provide a clean and safe environment in which you receive treatment and/ or care. By following the points in this advice, you can help us to prevent vulnerable individuals picking up an infection and prevent the spread of infections. If people pick up an infection, it can cause discomfort, pain and anxiety.
Health care associated infections (HCAIs)
What is an HCAI?
This is an infection that may affect people when they are receiving healthcare. People may catch these infections in hospitals, care homes, doctors’ surgeries, health centres and even at home if they are being cared for there.
Why do some people get an HCAI when receiving healthcare?
There are lots of reasons why someone can develop an HCAI. Being ill or receiving treatment can make your natural defence system (immune system) weaker than usual. Most people won’t pick up an HCAI while they are being treated but it is impossible to completely remove all the risk during healthcare. This is because every disease, condition or procedure and sometimes medication can reduce your natural defences against infection.
What are the most common types of HCAI in hospital?
The most common types of HCAI in hospitals are urine infections, wound infections, skin infections, chest infections and sickness and diarrhoea.
What type of germs cause HCAI?
Some are caused by germs that live normally on our bodies and usually do us no harm such as Staphylococcus aureus, which many people can carry harmlessly in their nose. The most well-known are methicillin resistant staphylococcus aureus (MRSA), clostridium difficile (c-diff) and norovirus.
MRSA can cause an infection if it gets into a wound, the bloodstream, bladder or lungs.
C-diff is bacteria that some people have living naturally in their bowel. For some people unfortunately, this can develop into diarrhoea and fever and usually after certain kinds of antibiotics.
Norovirus causes sickness and diarrhoea. This may last for a couple of days and usually has no lasting effects. This virus is often reported as causing outbreaks of infection in hospitals and care homes.
What do we do to prevent HCAIs spreading?
Preventing and controlling HCAI is a national priority and all care settings are working hard to prevent the spread of infection in the NHS and care homes. This includes:
- educating staff, patients and visitors on how to prevent and control infections, for example, washing hands regularly; getting support and advice from specialist infection control or health protection staff
- making sure that the NHS and care homes meet government standards on HCAI
- giving people information on how to prevent and control HCAI within all care settings and among members of the public
HCAIs are monitored and reported to Public Health England, for learning and improvement purposes.
What happens if I get an infection?
Your infection could require treatment, which probably can be given to you at home. You may be asked to stay at home for the duration of the treatment and not visit the GP surgery, they may arrange a home visit instead. If you don’t understand your condition and/or treatment please ask a member of staff.
Hydration
Dehydration is a state in which our bodies do not have enough water. NHS England defines dehydration as a relative deficiency of fluid that causes adverse effects on function and clinical outcome. Dehydration can be mild, moderate or severe.
Several poor health outcomes are associated with avoidable dehydration including some infections.
Dehydration should always be considered as a cause for any of the following:
- dry mouth, feeling thirsty
- headache, poor concentration, unexpected confusion, increasing agitation
- feeling dizzy when standing up
- lethargy, malaise, increasing sleepiness
- noticeably drier inelastic skin
- dark concentrated urine
- reduced urine output
Are you drinking enough?
A good rule is to drink enough fluid so that you’re not thirsty for long periods, and to steadily increase your fluid intake when exercising and during hot weather. Passing clear urine (wee) is a good sign that you’re well hydrated.
Try to drink six to eight glasses daily of fluids such as water or diluted squash. These are much more effective than large amounts of tea, coffee or fizzy drinks, which contain caffeine.
Links to patient information leaflets
- RCHT Clostridium difficile patient information
- RCHT GDH positive toxin negative patient information
- RCHT extended spectrum beta lactamase (ESBL), AmpC and K1 patient information
- RCHT Glycopeptide Resistant Enterococci GRE patient information
- RCHT Hand hygiene patient and visitor information
- RCHT MRSA patient information
- RCHT Norovirus (Winter vomiting virus) patient information
Vaccination
Vaccines are the most effective way to prevent infection diseases. They are the most important thing that we can do to protect ourselves and our children against ill health. They prevent up to 3 million deaths worldwide every year.
Since vaccines were introduced in the UK, diseases like smallpox, polio and tetanus that used to kill or disable millions of people are either gone or very rare.
Other diseases like measures and diphtheria have been reduced by up to 99.9% since their vaccines were introduced. However, if people stop having vaccines, it’s possible for infectious diseases to quickly spread again.
Vaccine hesitancy is where people with access to vaccines delay or refuse the vaccination. The World Health Organisation (WHO) recently listed vaccine hesitancy as 1 of their top 10 biggest threats to global health.
How do vaccines work?
Vaccines teach your immune system how to create antibodies that protect you from diseases. It’s much safer for your immune system to learn this thought vaccination than by catching the diseases and treating them. Once your immune system knows how to fight a disease, it can often protect you for many years.
Are vaccines safe?
All vaccines are thoroughly tested to ensure that they won’t harm you or your child. It often takes many years for a vaccine to make it through the trials and tests it needs to pass for approval. Once a vaccine is being used in the UK it’s also monitored for any rare side effects by the Medicines and Healthcare Products Regulatory Agency (MHRA).
What’s in a vaccine?
Most people aren’t concerned about vaccine ingredients and know that they’re safe. The main ingredient of any vaccine is a small amount of bacteria, virus or toxin that’s been weakened or destroyed in a laboratory first; this means there’s no risk of healthy people catching a disease from a vaccine. It’s also why you might see vaccines being called live or killed vaccines.
Pneumococcal vaccine
The pneumococcal vaccine helps protect against serious pneumococcal infections, which can lead to pneumonia, septicaemia (a kind of blood poisoning) and meningitis. In some cases they can lead to permanent brain damage, or even death.
A pneumococcal infection can affect anyone. Some people are at higher risk of serious illness and can get the pneumococcal vaccine free from the NHS.
Who is eligible for the free vaccine?
- Adults aged 65 or older need a single pneumococcal immunisation, which will help protect them for life.
- Children younger than 2 years are offered doses of the vaccine as part of the routine childhood immunisation programme. Some children with a health condition, older than 2 years, may require additional doses.
- People with long term conditions usually need a single 1 off immunisation or 5 yearly immunisation, depending on their underlying health condition.
What is pneumococcal infection?
This infection is caused by pneumococcal bacteria. It can cause serious illness, such as pneumonia and meningitis.
How is pneumococcal infection spread?
Some adults and up to 60% of children, carry the bacteria in the back of their nose and throat, and can pass them around by coughing, sneezing and close contact. Usually this doesn’t result in serious illness.
Why should I worry about pneumococcal infection?
Pneumococcal infection can cause bronchitis, ear and sinus infections, life-threatening infection of the blood (septicaemia), meningitis and pneumonia (which can also be life-threatening).
Children younger than 2 years of age, people aged 65 or older, and children and adults with certain health conditions have a higher chance of becoming unwell with pneumococcal infection. People aged 65 or older are more likely to suffer serious long-term health problems, and can even die.
How serious is pneumococcal meningitis?
About 85% of people who get pneumococcal meningitis recover, usually without any long-term problems. Survivors of pneumococcal meningitis, however, are more likely to develop complications than survivors of other bacterial causes of meningitis. These complications include deafness, seizures and long-term brain damage.
Who should get the vaccine?
The pneumococcal vaccine is recommended for many of the same people who get an annual flu vaccine.
Pneumococcal immunisation is available in the England for all people aged 65 years and older. For anyone younger than 65, including children, GPs may provide immunisation for people with the following serious medical conditions:
- problems with the spleen, either because the spleen has been removed or doesn’t work properly
- chronic lung disease, including chronic bronchitis or emphysema
- serious heart conditions
- severe kidney disease
- long-term liver disease
- diabetes that require medication
- lowered immunity due to disease or treatment (people with HIV, receiving chemotherapy, or are on long-term oral steroids)
- cochlear implants
- cerebrospinal fluid leaks
- children younger than 5 years who have previously had invasive pneumococcal disease, such as meningitis or bacteraemia (presence of bacteria in the blood)
If you’re unsure whether you or your child should get the vaccine, speak to your GP or practice nurse.
Why shouldn’t everyone have the pneumococcal vaccine?
Not everyone is at high risk of developing serious illness. The maximum risk is in those aged 65 or older, and those younger than 65 with any of the serious medical conditions listed. Children younger than 2 years are also at increased risk.
Does the vaccine have any possible side effects?
The pneumococcal vaccine is very safe. Although, like all vaccinations, it can cause side effects. It’s not possible to catch a pneumococcal infection from the vaccine, as the vaccine does not contain any live bacteria.
Possible side effects in babies:
- a decreased appetite
- a slightly raised temperature
- irritability
- redness and swelling at the site of the injection
- feeling sleepy or not sleeping well
Side effects in adults and children older than 2:
- mild soreness or hardness at the site of the injection lasting 1 to 3 days
- a slightly raised temperature
More serious side effects of the vaccine, such as allergic reactions, are rare. Contact NHS 111 if you’re concerned.
How effective is the vaccine?
Getting the vaccine is the best way to help protect yourself against infections caused by the most common types of pneumococcal bacteria. It doesn’t protect you against infections caused by all pneumococcal bacteria.
How safe is the vaccine?
Before they are allowed to be used, all medicines (including vaccines) are tested to assess their safety and effectiveness. Once they have been licensed for use, their safety continues to be monitored.
Vaccine allergy
Tell your GP if you, or your child, has had a bad reaction to any vaccination in the past.
If there’s been a confirmed severe allergic reaction, called an anaphylactic reaction, to the pneumococcal vaccine or any ingredient in the vaccine, it may not be possible for you to have it. If it was only a mild reaction, such as a rash, it’s generally safe to have the vaccine.
Report side effects
You can report suspected side effects online on the Yellow Card website. You can also call the Yellow Card hotline on 0808 100 3352.
Where can I get more information
Visit nhs.uk for more information. You can also talk to your practice nurse or GP, or contact NHS 111.
Say no to norovirus
Norovirus affects everyone. It can close hospitals, care homes and schools. It is the most common cause of stomach bugs in England and Wales.
How does norovirus spread?
Norovirus can be caught from contact with an infected person:
- by consuming contaminated food or water
- contact with contaminated surfaces or objects
What are noroviruses?
They are a group of viruses that are the most common cause of stomach bugs in England and Wales. In the past, noroviruses have also been called the winter vomiting virus or Norwalk virus.
What are the symptoms?
Symptoms begin around 12 to 48 hours after you become infected and can last for 12 to 60 hours. They start with the sudden onset of nausea followed by projectile vomiting and watery diarrhoea. Some people will have a raised temperature, headaches and aching limbs. Most make a full recovery within 1 to 2 days. Some people, usually the very young or elderly, may require rehydration treatment, either at home on in hospital.
Why does norovirus often cause outbreaks?
Norovirus is easily spread from 1 person to another. The virus is able to survive in the environment for many days. As there are many different strains, immunity is short-lived. Outbreaks tend to affect more than half of susceptible people. They usually happen in semi-closed environments like nursing homes, hospitals, schools and cruise ships.
How can these outbreaks be stopped?
Outbreaks can be difficult to control and long-lasting because the virus is easily transmitted and survives in the environment for a long time.
The most effective way to help stop an outbreak, is to disinfect the contaminated areas and ensure good hygiene. For example thorough handwashing and good food hygiene. Alcohol gel is not effective against norovirus.
Anyone who has the symptoms should be isolated or avoid contact with others for a minimum of 48 hours after their symptoms have stopped. Those affected should not go to work or school until they have been symptom free for 48 hours.
How is norovirus treated?
There is no specific treatment for norovirus apart from letting the illness run its course. It is important to drink plenty of fluids to prevent dehydration. Medical advice should be sought if symptoms do not resolve themselves.
Why does norovirus close hospitals?
Although norovirus doesn’t start in hospitals, if brought in from the community, it can make people who are already very ill even more poorly.
Who is at risk of getting norovirus?
People of all ages can be infected. The very young and the elderly should take extra care if infected, as dehydration is more common in these age groups. Outbreaks can be shortened when control measures are implemented quickly. This will include closing infected areas and using strict hygiene measures.
Are there any long-term effects?
There are no long-term effects from norovirus.
What you can do to help us stop the infection
Do not visit health care settings if you, or someone you’ve been in contact with, has had diarrhoea and/or vomiting until 48 hours after symptoms have ceased. There is a real risk that you could introduce the infection into the area.
Wash your hands frequently with warm water and liquid soap, especially after using the toilet and before preparing food. Alcohol gel is not effective against norovirus.
If you’re concerned about the health of the person you are visiting, speak to a member of staff.
Do not handle or prepare food for other people until you have been symptom free for a minimum of 48 hours.
Urinary tract infections
Urinary tract infections are common infections that can affect the bladder (cystitis), the kidneys and the tubes connected to them.
Anyone can get them, but they’re particularly common in women. Some women experience them regularly (called recurrent UTIs).
Urinary tract infection (UTIs) are the second most common type of infection that can occur in the body and are usually caused by bacteria that enter the body via the urethra (tube that carries urine out of the body).
Symptoms of UTIs
Infections of the bladder or urethra are known as lower UTIs. These can cause (not always all of these together):
- needing to urinate (wee) more often and urgently than normal
- pain, burning or stinging when you wee
- feeling as though you’re unable to empty your bladder fully
- urine that’s dark, cloudy or strong-smelling
- feeling generally unwell, achy and tired
Infections of the kidneys or ureters are known as upper UTIs. These can cause the above symptoms and also:
- a high temperature (fever) of 38ºC (100.4ºF) or above
- pain in your sides or back
- shivering and chills
- feeling and being sick
- confusion, agitation or restlessness
Lower UTIs are common and aren’t usually a cause for major concern. Upper UTIs can be serious if left untreated. If symptoms don’t improve or you are worried, contact your pharmacist, GP or contact NHS 111.
Treatment of UTIs
Mild cases often get better by themselves within a few days. Symptoms of cystitis can also be caused by other conditions, so children and men should always see their GP.
Over-the-counter painkillers such as paracetamol can help with any pain. Drinking fluids may also help you feel better. There’s currently little evidence to suggest that drinking cranberry juice significantly reduces your chances of getting UTIs.
Avoiding sex when you have a UTI may also help because it may make the condition worse.
If symptoms persist, talk to your pharmacist who can assess your symptoms and advise on appropriate treatments. This may involve testing a sample of your urine. You can also contact NHS 111 for advice.
Preventing UTIs
If you get UTIs frequently, there are some things you can try that may stop it coming back.
- Staying well hydrated (drink six to eight glasses of water daily).
- Avoiding perfumed bubble bath, soap or talcum powder around your genitals – use plain, unperfumed varieties, and have a shower rather than a bath.
- Going to the toilet as soon as you need to wee.
- Wiping your bottom front to back when you go to the toilet.
- Emptying your bladder as soon as possible after having sex.
- Not using a contraceptive diaphragm or condoms with spermicidal lubricant on them – consider using alternative products or methods.
- Wearing underwear made from cotton, rather than synthetic material such as nylon, and avoiding tight jeans and trousers.
For further information, please see below UKHSA resources:
Page last reviewed: 17 July 2024